
“He was the only one able to run X-rays, and without the service the ER was at risk of closing.” – Business Insider
Captain Obvious Visits Healthcare
A recent article in the Business Insider explains how a lone radiographer had to sleep in an RV on-site in order to keep a hospital open.
His presence was essential because you can’t run a hospital without radiology services. 9 out of 10 patients need either lab work or imaging, or both, to help the physician figure out what is wrong with the patient.
How this has gone unrealized for so long is beyond me. There are some positions inside of healthcare that you simply cannot operate a hospital without:
- Physicians
- Radiologic Technologists (Rad Techs)
- Medical Technicians (Med Techs)
- Respiratory Therapists (RTs)
….and that’s about it.
What?! What about nurses, environmental services and on and on.
Think about it. Be honest with yourself. Is a nurse trained to do what a physician does?

No.
But is a physician trained to do what a nurse does? If you’re struggling to answer that, let’s talk that through:
- Give medications? Yes, physicians write the prescriptions based on years of pharmacology classes.
- Start IVs and hang medication bags. Yep. Even better, physicians are trained to start any “type” of line they want: arterial, venous, subclavian, intrajugular, midline, picc line, and so on.
- Clean up after patients. Is their time better spent somewhere else…yes. But could they do it. Yep.
I think I’ve made my point. It’s extreme, I know.
Listen.
Do we want nurses in healthcare…absolutely. They allow doctors to treat more patients.
Nurses serve as an extension to the physician.
But let’s talk extreme cases.
An entire hospital nursing base goes on strike. What happens next?
Administration instructs Human Resources to temporarily hire travel nurses to come in and take over until a resolution can be resolved.
This model works because nursing is nursing. The skills are transferable. Nurses don’t have to worry about showing up at a hospital and seeing three different CT scanners purchased and manufactured by three different vendors.
$200 IV pumps are no where near as complicated as a $1.5 Million dollar CT scanner.
We’ve seen nurses go on strike before. It’s nothing new. Life goes on.
Laboratories are Sending out Blood Work
More and more blood tests are being centralized at one laboratory “hub.” Call it the Spoke and Hub model, call it the UPS model, call it whatever you want.
Less and less blood tests are being performed in-house because it is cheaper to buy one laboratory worth of expensive testing equipment and centrally locate it.
Then use the carriers, the transporter cars, to pick up specimens every 30 minutes and drive them to the hub.
For ER labs that are needed STAT, tests are slowly becoming test strips read immediatley on the spot…like Rapid Strep Tests and glucometers reading blood glucose off of a drop of blood on the end of a test strip.
Medical Laboratory Technicians are slowly being outsourced to the “central lab” or to the 3rd party commercial lab like Quest Labs.
Many departments already draw their own blood samples and transport them to the lab, slowly eliminating the need for phlebotomists.
Numerous hospitals are now outsourcing Food and Nutrition (cafeteria workers), Security, Environmental Services, Billing and Coding, Central Scheduling and more.
Cross Training at the Core
So physicians can perform nursing duties, venipuncture for the lab, and even delve into the art of reading or interpreting basic radiology images.
If it is a complicated study, like an MRI, it gets sent out for a read to a third party.
But nobody…NOBODY is trained on how to operate radiology equipment except for radiologic technologists. Not even radiologists know the first thing about performing a CT scan or even obtaining a general xray.
And you can’t do it remotely. You can’t send your ER patient ten miles away to an outpatient imaging center for a CT scan and then transport them back to the hospital.
Radiology is what you call an essential service.
Did you know that on top of being specialists at operating million dollar equipment, radiologic technologists are also trained to obtain vitals and start IVs?
Rad Techs are taught venipuncture in school and how to obtain blood pressures, pulses, respirations, and temperatures.
That means a Rad Tech can take the place of a Certified Nursing Assistant, Certified Medical Assistant, and if you really want to get technical, can give medications similar to a nurse.
Why?
Rad Techs are trained and certified to start intravenous lines and administer contrast agents of varying medicinal properties. Giving ionic, non-ionic, oral, intravenous, and rectal contrast medications are some of the common duties of a rad tech.
Now you might be educated enough to say “Ah, the techs can obtain the images but they are practicing outside of their scope if they try to interpret the images.”
And you would be correct. But they can be outsourced. Therefore, radiologists fall into the non-essentials, at least…not essential to be at the hospital. Most of them would rather read from home anyway.
Radiology images can get sent out to third party reading companies…and quite often do. Many hospitals employ reading services to cover overnight services so their radiologists can enjoy a night off.
It is very commonplace for radiologists to have “reading stations” at their home so they can do their job from home. It simply isn’t essential for them to be onsite to read studies.
The Radiologic Technologists Hold the Keys
So the physicians are the captains of the healthcare ship. But more times than not, they need medical imaging to find out what is going on inside the patient.
Labs can be collected and sent out. Intubations and breathing machines can be started by the physicians if RTs aren’t available.
But the Xrays, CT scans, MRIs, Ultrasounds, Nuclear Medicine Scans, PET scans and Mammography are all peformed by one skilled, specialized employee…the Radiologic Technologist.
Don’t believe me? Ever see an imaging department go on strike? Nope.
The hospital would cease to function...just like the Business Insider article points out.
But let’s say it does. Let’s say Administration treats the imaging employees poorly long enough that a strike of imaging techs occurs.
Traveling techs can be brought in. You think traveling nurses eat up your budget? Try a travel MRI Tech for one month. It would cost more than a pretty penny to hire temporary travel technologists.
But there are a minimum of half a dozen equipment manufacturers out there for one CT scanner, every MRI scanner, and even more vendors for general xray and ultrasound.
When radiology technologists are hired for regular full-time jobs, they are given at least one full month just to get familiar with the different equipment and layout of the hospital.
This is after a two-year unpaid clinical rotation which is spent working on various equipment to learn protocols and imaging techniques.
To think you can pull in traveling technologists during a strike that are going to know all the intricate details of every scanner AND perform exams in a timely and safe fashion is ridiculous and futile at best.
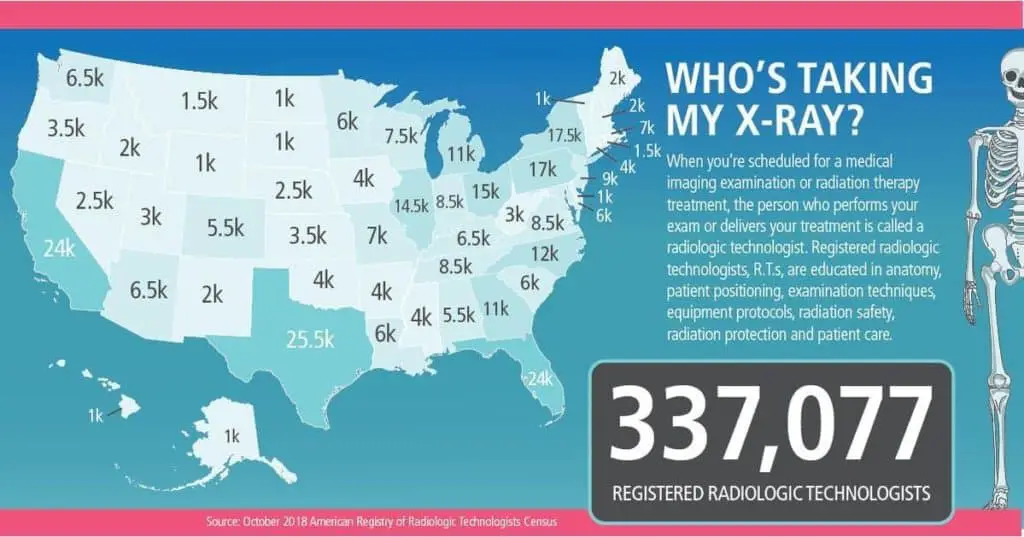
Not to mention that there is already a shortage of imaging technologists to begin with in our industry. A 200 bed hospital could easily employ 50 technologists on a daily basis.
After a decade of imaging administration, I’d be lucky to find TWO traveling technologists at the same time…let alone 50.
Fate Lies with the Adminstrators
We don’t really need to talk about how essential an administrator is to healthcare, right? Nobody is arguing that the hospital can’t run without the CEO.
In fact, I believe that is one of the most volatile positions in a hospital. You want to see high turnover? Look at the tenure of most hospitals’ CEOs, CNOs, COOs, CFOs.
It has always been the “frontline” that keeps the lights on.
So let’s hope that all those hospital administrators out there who keep cutting back staffing to be “more efficient” wake up.
The same administrators who keep delaying the replacement of end-of-life equipment because it is more important that a spoiled ortho surgeon gets a new O-Arm for his surgical suite.
And then have the audacity to blame the community for their woes because citizens aren’t sticking to CDC guidelines, thus causing an overflow of patients in the hospital.
It’s ludicris.
You cut the staffing to squeeze more profit from the department pre-Covid.
Forced the staff to burn their own Paid Time Off (PTO) hours so you could save a few bucks in your budget.
You refused advances from Tech I to Tech II or Tech II to Tech III because you didn’t want to pay more in hourly wages.
And now you wonder why staff morale is at an all-time low.
Let’s hope they start treating the radiologic technologists like they are essential and pay them accordingly.
They can’t feed their families with “Heroes Work Here” banners hanging outside of their facility.
A five-dollar gift card does not make up all the hours they’ve missed with their families to pick up extra shifts because the department is understaffed.
I’ll tell you what.
Here’s an idea.
Fire the CEOs and let somebody from Radiology run the hospital.
Because heaven help us if the radiologic technologists decide to strike.
