(8 Staffing Model Templates Attached)
(PPT Slides for Schedule Reduction Attached)
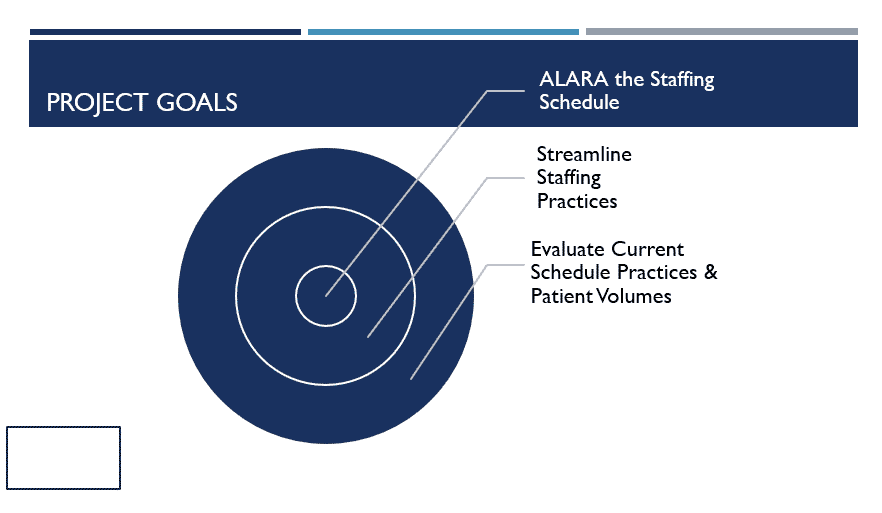
As Low As Reasonably Achievable now applies to staffing models and not just radiation levels.
The Coronavirus pandemic has reduced patient volumes in healthcare settings across the country.
While some emergency rooms and intensive care units are getting hammered with more patients than they can handle, other departments are a mere fraction of what they used to see daily.
Like imaging departments.
Particularly in critical access hospitals where volumes are already lower than those of their big city counterparts.
The Case for Cross-training Staff
I have touted for years the reasons why every imaging department should embrace cross-training. To see all the Pros and Cons, visit this article.
If you are one of the departments who only hired outside talent, you are now in a world of hurt.
The trouble you now face isn’t because you hired unqualified technologists. The trouble you are in now is that you can’t afford to have a uni-modality technologist sitting around during low volumes.
Had you cross-trained your staff, you could get by with fewer techs during times of crisis like these.
Fiscally Responsible to Reduce Staffing
According to this article, imaging departments can expect to see a 50-70% decrease in volumes for at least three or four months.
That’s INSANE!
This is the outcome of the distancing measures we have taken to slow the transmission of the Covid-19 virus.
The only way to counter-balance the reduction in revenue is to reduce expenses. The biggest expenses in any imaging department is equipment and staffing.
And we can’t furlough the CT scanner.
So, what is the best method to reduce staffing in a situation like this?
7 Tips for a Successful Staffing Reduction Plan
1. Share the burden evenly
My wife is a radiographer for a large hospital system. She works in the outpatient side of the hospital and services the Quick Care and physician offices over there.
When volumes began to drop a few years ago, technologists started receiving orders to go home. She was told she had to clock out early and if she wanted to get paid, use her PTO.
Only the locations experiencing the low volumes were targeted.
One month later, she had used all of her PTO to help the hospital save hours. That is NOT what PTO is designed to do. PTO is earned by employees to take time off from work when the employee chooses to do so.
Needless to say, it wasn’t until she pointed out that all of her PTO was gone that her supervisor realized he needed to share the burden among the rest of the 35+ technologists.
Don’t be that leader!
Review your entire staff and be aware of who can float to different locations. Outpatient technologists can work the inpatient main department…unless you never cross-trained them.
Offer a Sign Up Sheet where technologists can opt to go home early when the need arises. Once that list is exhausted, send employees home in a fair and equal manner.
I am also a proponent of allowing employees to use Long Term Sickness or Extended Illness Benefits during times like this. But ultimately, it is up to senior administration.
2. Make Sure All Modalities are Reasonably Covered
General radiography and CT need to remain the key focus. Ultrasounds, depending on your location, can be reduced on the schedule to a few days each week or take them as on-call. The same goes for MRI.
Of course, this all depends on your volumes and your individual location. It will also depend on what your technologists can cover.
Non-emergent exams will most likely be rescheduled until the mandated distancing model is revoked.
This includes screening mammograms, DEXA scans, elective IR and OR procedures, etc.
3. Keep Your Eye on the Call
Staff will most likely lose some working hours during their normal shifts. But the call hours are likely to increase.
Keep an eye on how many callbacks are being performed and who is doing them. Don’t wait until it is too late to find out only a few techs have been stuck doing most of the callbacks.
Excessive or an unexpected increase in callbacks is one of the top reasons for tech burnout. For more on technologist burnout, see my in-depth article here.
Share the burden of being on-call evenly just like you do with flexing out early.
There is also a safety factor here when techs get called in at night and then report for duty the next morning.
4. By All Means, Ask for Tech Input
There are two types of technologists out there: those who are resistant to change and those who can mitigate it.
Notice I didn’t say they liked it. I said they can mitigate it. Actually, they handle change better when they have a sense of control over it. Wouldn’t you?
Asking staff to collaborate and come up with their own modified reduced schedule decreases resistance to the new schedule and garners “buy-in.”
If the staff has bought into the new schedule, everything will go much smoother.
5. Look for Alternative Hours Outside of Imaging
You may have to ask staff to reduce shift hours due to low volumes. Most already have. But are there other areas in the facility that can use extra help?
Most hospitals have reduced the points-of-entry into the hospital to one or two entrances. This helps in controlling who goes in and out of the hospital.
These “check points” are also being used to evaluate everyone who enters. An average temporal temperature scan and a few questions successfully answered gets you permission to enter the hospital.
These door guards can be anyone who can take a temperature and ask a few questions. Plus, hospitals can’t afford to put CNAs and RNs in these positions because they are desperately needed in the ED and units.
Ask if your radiology staff can sign up for hours helping at these checkpoints. The hours typically don’t get charged to your imaging department either. They get charged to a general account with hopes that some federal aid is coming to help offset.
Also, many regulations require certain patients to have assigned “sitters” in their room to keep an eye on them. Whether it is a fall risk patient or suicidal ideation, there is often a shortage of sitters in the hospitals.
Ask if your staff can access these hours and get on a schedule to fill in when needed.
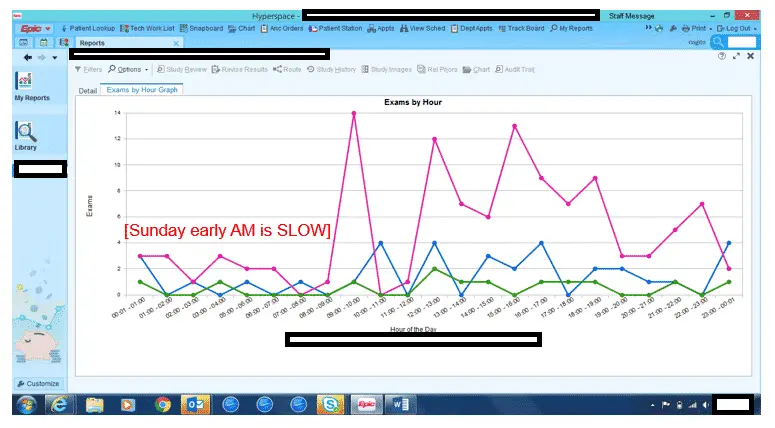
6. Use a HotSpot Report to Staff When Needed
These reports go by many names but their purpose is simple: determine the busiest times of each day.
I run these reports for every day of the week. Saturday and Sunday have a completely different pattern than weekdays.
There are also seasonal swings as well. A ski resort town looks completely different in the summer months than it does in the winter.
Don’t forget to reduce staff on holidays as well. It is usually a safe bet to reduce staff the day before and the day after a holiday, depending on which day of the week the holiday falls.
Sometimes even the whole holiday week, like for Christmas.
7. Keep Copies of All Clinic Hours
When physicians schedule vacation time, you need to know. This is a key time to reduce staff for that particular area.
Is your Pediatric Clinic going to lose three of the four Pediatricians over Spring Break? If you have dedicated technologists in their area, you will not want to fully staff during that time frame or your expense reports will look horrible.
Ask that office managers keep you up-to-date with the latest clinic schedules. If you are really lucky, these are online and you can check them easily.
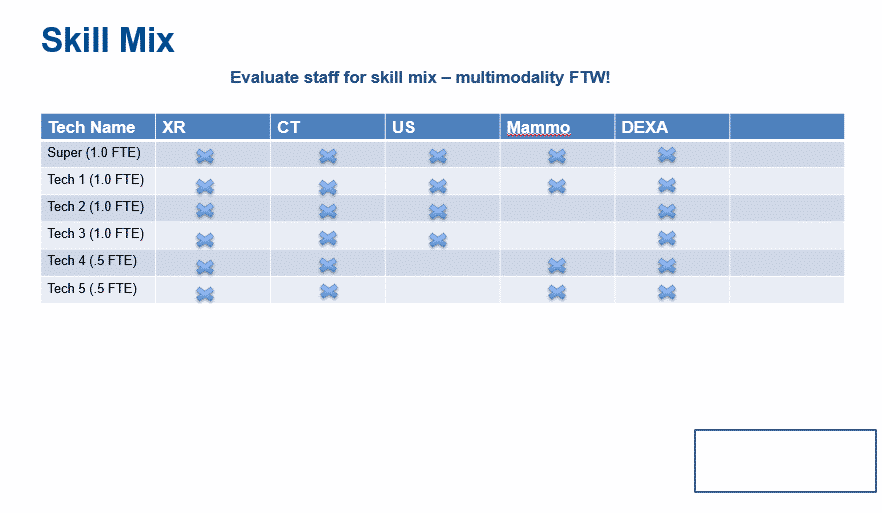
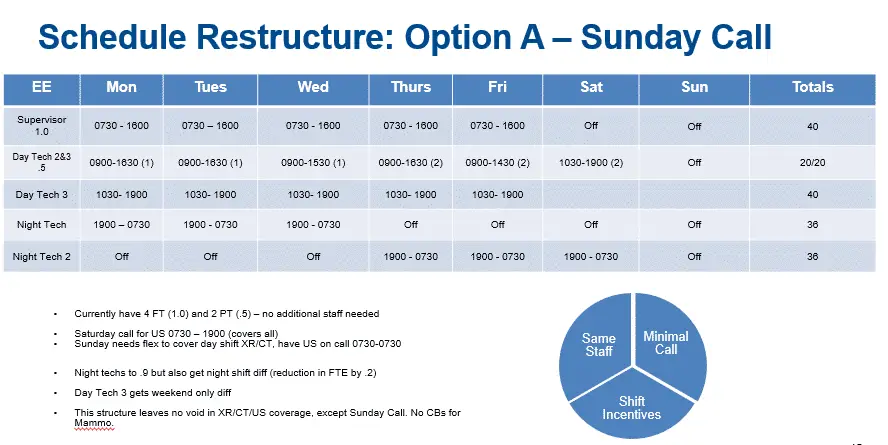
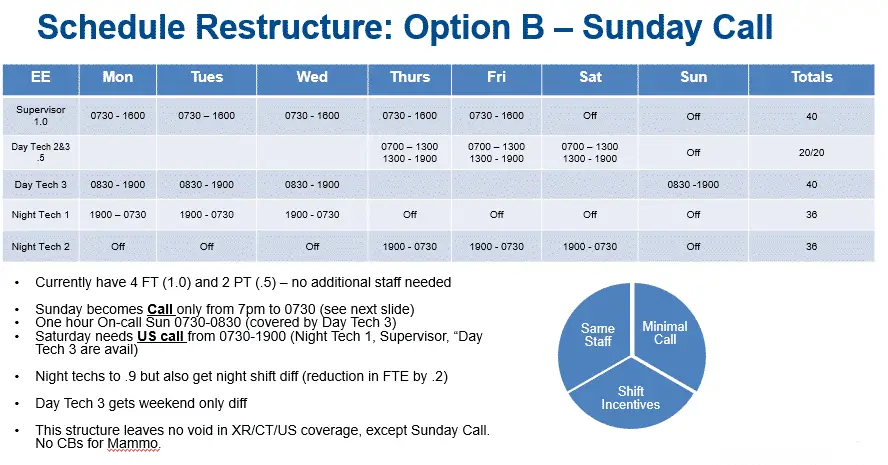
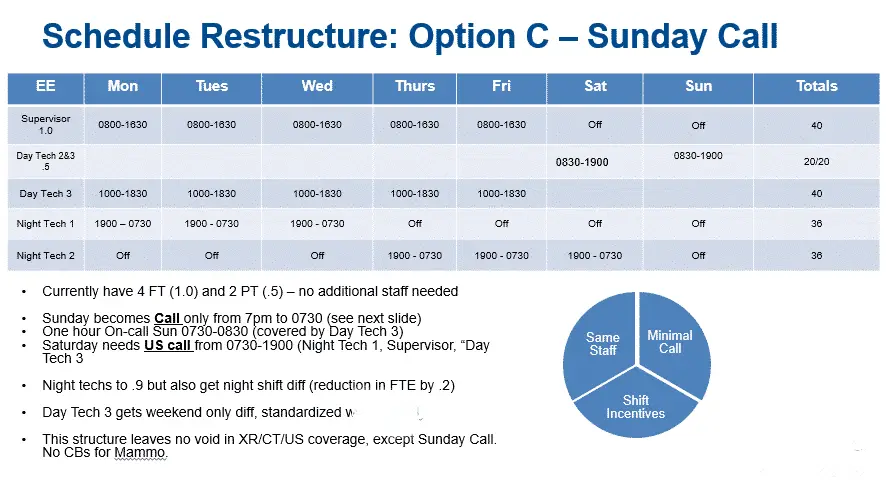
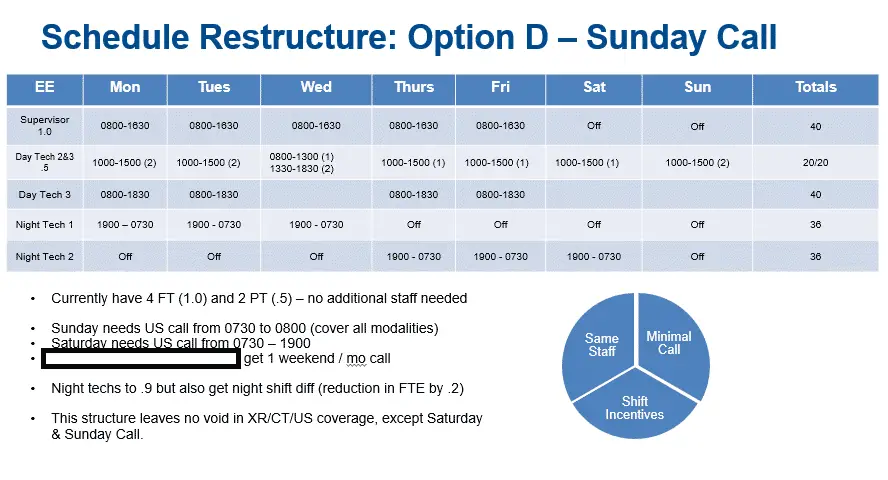
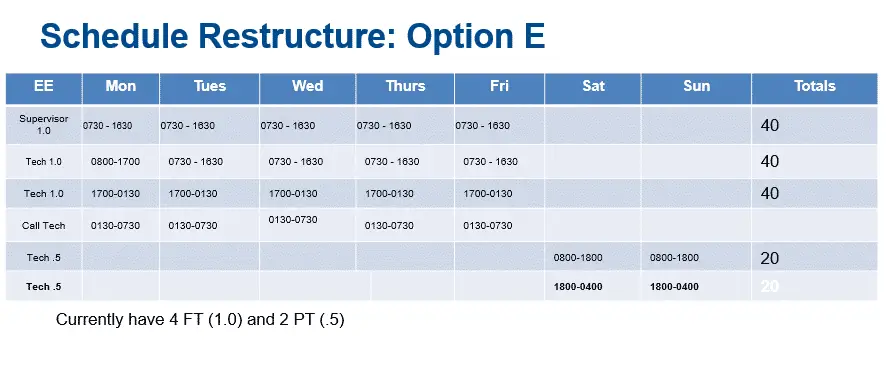
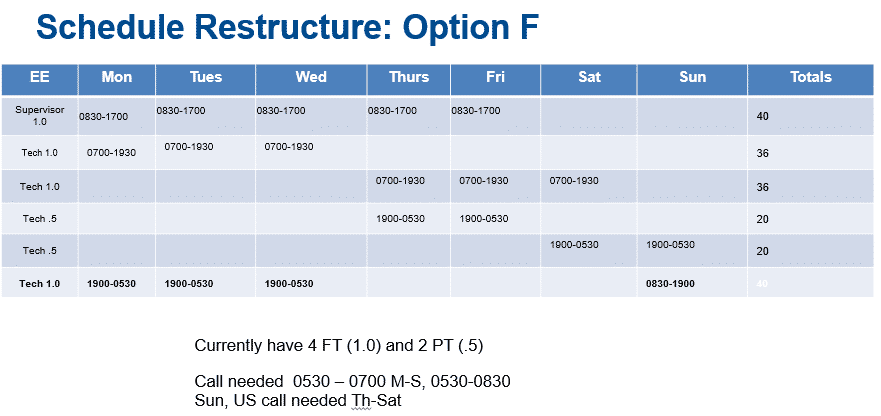
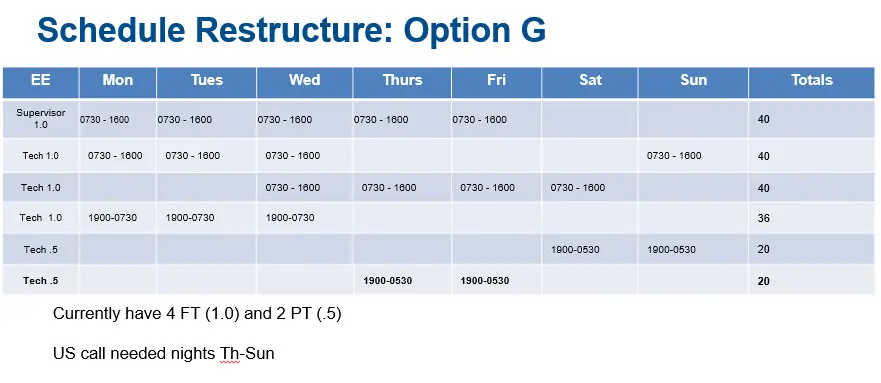
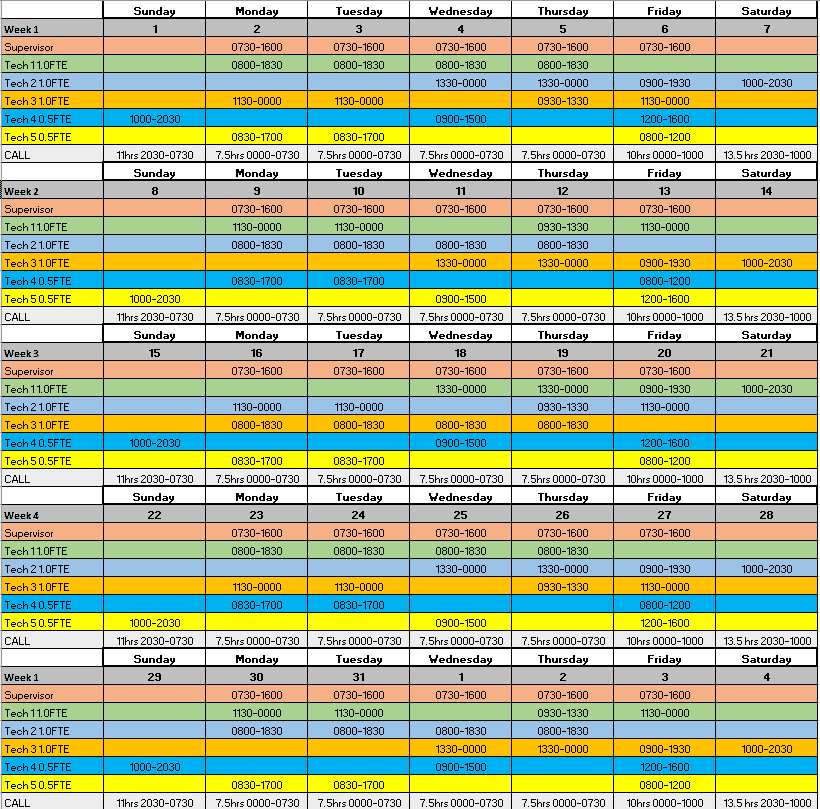
8 Common Staffing Templates
I will share the staffing templates I have considered in the past few years when reorganizing and reducing hours.
They are for critical access hospital departments so they won’t apply to large imaging departments. This location had one supervisor, three full-time FTEs and two part-time FTEs that were both .5 FTE.
Although, it might be a drastically different setup than yours, it may give you ideas to get you to a working staffing model that makes sense for your department.
There are dozens of ways to configure these shifts. Cover nights or only offer call at night. Shifts on weekends or only on call.
Use your HotSpot reports to determine the best coverage.
These schedules are for a CAH with XR, CT, US, Mammo, & Dexa. MRI was covered by the company that provided us with a mobile MRI scanner. No IR, PET or NM on campus.
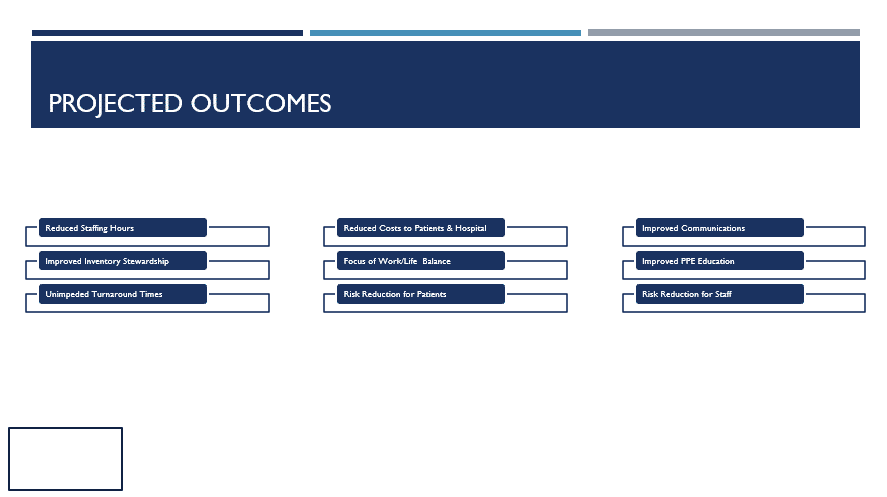
Conclusion
I hope this article helps give you some ideas on how you can modify your staffing schedule during these difficult times.
Don’t forget to evenly distribute any reductions and keep your eye on work/life balance.
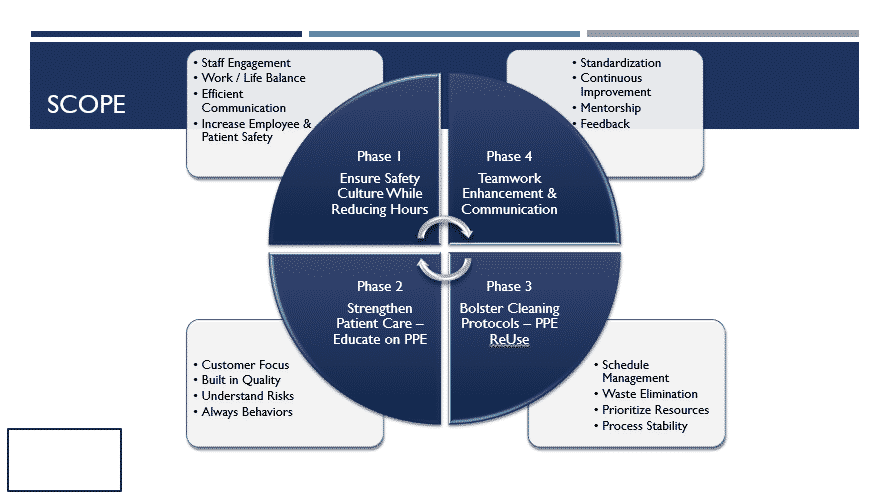
If you need to pull together a ppt, here’s some of my slides from past restructures.